Why Confidence Matters After Scrotal Reduction
Scrotoplasty reshapes the scrotum by removing excess skin and tissue, resulting in a firmer, more proportionate organ. The physical change reduces chafing, bulk, and visual discrepancies that can cause discomfort during intercourse, allowing smoother movement and less distraction. Because the scrotum now looks and feels more natural, men often experience a boost in body image and self‑esteem; the aesthetic improvement aligns the genital appearance with personal expectations, lowering anxiety about appearance in intimate settings. This uplift in confidence directly influences sexual satisfaction—confidence promotes relaxation, reduces performance pressure, and encourages open communication with a partner. When men feel comfortable with their bodies, they are more likely to engage in intimacy, experiment with positions, and experience higher libido and erection quality. In summary, the physical benefits of scrotoplasty translate into psychological gains that together enhance overall sexual well‑being.
Healing the Body: Post‑Operative Care and Physical Recovery
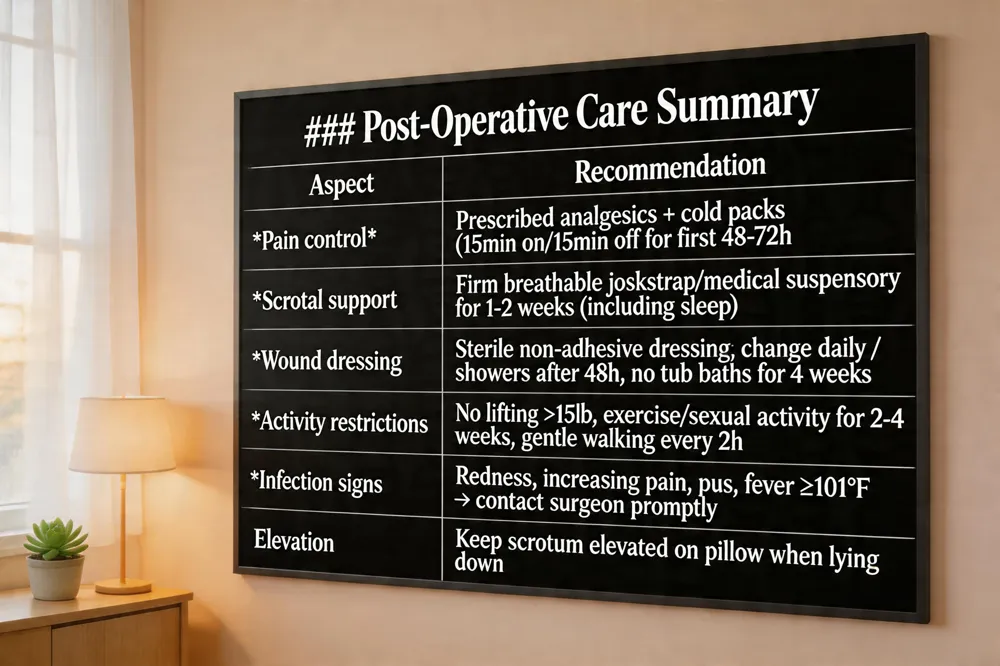 Swelling, bruising, and pain are normal after orchiectomy or scrotal reduction. Expect mild‑to‑moderate discomfort for the first 1‑2 weeks; manage it with prescribed analgesics, cold packs (15 min on/15 min off for the first 48‑72 hours), and keep the scrotum elevated on a pillow when lying down.
Support garments are essential. Wear a firm, breathable jockstrap or medical‑grade suspensory support continuously for the first 1‑2 weeks, even while sleeping, to immobilize the area, reduce edema, and protect incisions. Choose a size‑specific pocket or adjustable straps to avoid circulation compromise.
Wound dressing should be sterile, non‑adhesive, and changed daily or when saturated. Keep the incision clean and dry; showers are permissible after 48 hours, but avoid tub baths for at least four weeks. Watch for infection signs—redness spreading beyond the incision, increasing pain, warmth, purulent discharge, or fever ≥101 °F—and contact your surgeon promptly.
Activity restrictions include no heavy lifting (>15 lb), vigorous exercise, or sexual activity for at least 2‑4 weeks, depending on surgeon clearance. Gentle walking every two hours promotes circulation without stressing the surgical site.
By adhering to these guidelines—proper pain control, consistent scrotal support, meticulous wound care, and activity limitations—you facilitate optimal tissue healing, minimize complications, and lay the groundwork for a confident return to intimate life.
Hormones, Fertility, and the Body’s Natural Balance
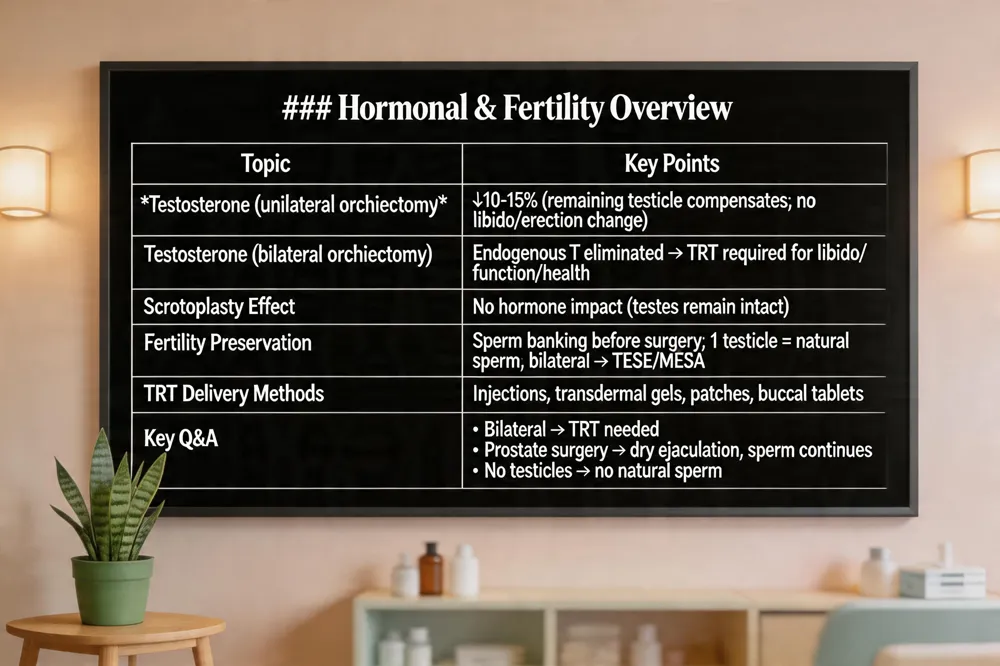 Testosterone changes after orchiectomy and scrotoplasty Unilateral orchiectomy usually lowers circulating testosterone by only 10‑15 % because the remaining testicle compensates; most men notice no change in libido or erection quality. Bilateral orchiectomy eliminates endogenous testosterone, making testosterone replacement therapy (TRT) essential for preserving sexual desire, erectile function, muscle mass and bone density. Scrotoplasty does not affect hormone production, as testicles remain intact.
Fertility preservation and sperm banking Before any testicular or scrotal surgery, sperm banking is strongly advised. If one testicle remains, natural sperm production typically continues; however, bilateral removal stops sperm creation entirely, requiring assisted‑reproductive techniques such as TESE or MESA if future fertility is desired.
Impact on libido and erectile function Hormonal drops after orchiectomy can reduce libido, but TRT restores sexual drive in most cases. Erectile dysfunction, if present, responds well to PDE‑5 inhibitors, pelvic‑floor training, or vacuum devices. Psychological support, open partner communication, and body‑image counseling further boost sexual confidence after both orchiectomy and scrotoplasty.
Answers to key questions:
- Removing one testicle lowers testosterone modestly; levels should be monitored.
- After double orchiectomy, TRT is required to maintain hormonal balance.
- Prostate surgery does not stop sperm production, though ejaculation becomes dry.
- No testicles mean no natural sperm.
- TRT can be delivered via injections, gels, patches, or buccal tablets.
- Orchiectomy does not affect life expectancy; outcomes depend on the underlying disease.
Restoring Erectile Function: Medical and Rehabilitation Strategies
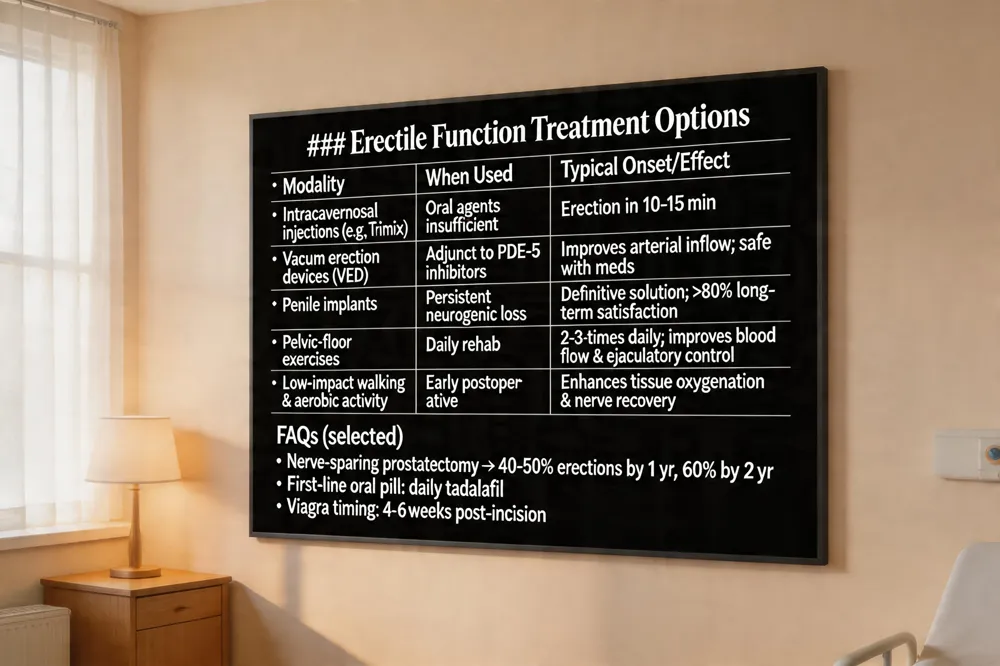 Penile Injections, Vacuum Devices, and Implants – When oral agents are insufficient, intracavernosal injections (e.g., Trimix) provide reliable erections within 10‑15 minutes. Vacuum erection devices (VEDs) enhance arterial inflow and can be used safely alongside PDE‑5 inhibitors. For men with persistent neurogenic loss, a penile implant offers a definitive solution, with satisfaction rates exceeding 80 % in long‑term studies.
Pelvic‑Floor Exercises and Nerve Regeneration – Gentle Pelvic‑Floor Exercises performed 2‑3 times daily improve pelvic blood flow, support erection quality, and aid ejaculatory control. Early, low‑impact walking and progressive aerobic activity promote tissue oxygenation and may accelerate nerve recovery after radical prostatectomy or scrotal reduction surgery.
FAQs
- Can you still get an erection after prostate removal? Yes; nerve‑sparing surgery preserves cavernous nerves in 40‑50 % of men within a year, rising to 60 % by two years.
- What is the best pill for post‑prostatectomy ED? Tadalafil is widely favored for its daily dosing convenience.
- How often should I take Viagra after prostatectomy? A daily low‑dose PDE‑5 inhibitor (e.g., 5 mg tadalafil) is commonly prescribed for the first 6‑12 months.
- How soon can you take Viagra after prostate surgery? Typically after the incision has healed, about 4‑6 weeks.
- Injections for erectile dysfunction after prostate surgery – Trimix (alprostadil, papaverine, phentolamine) is the standard formulation.
- How long does erectile dysfunction last after prostate surgery? Most men improve within the first year; 40‑50 % recover pre‑operative function, increasing to 30‑60 % by year two.
- Why can't I get hard after surgery? Nerve irritation, vascular disruption, hormonal shifts, and stress can transiently impair erections.
- Can I walk after testicular surgery? Begin with short walks, gradually increasing distance to boost circulation.
- Can I poop after testicular torsion surgery? Maintain regular, fiber‑rich bowel movements to avoid straining.
- Can testicular surgery cause erectile dysfunction? Unilateral orchiectomy usually preserves testosterone and erections; bilateral removal often requires testosterone replacement to prevent ED.
Psychological Resilience and Partner Communication
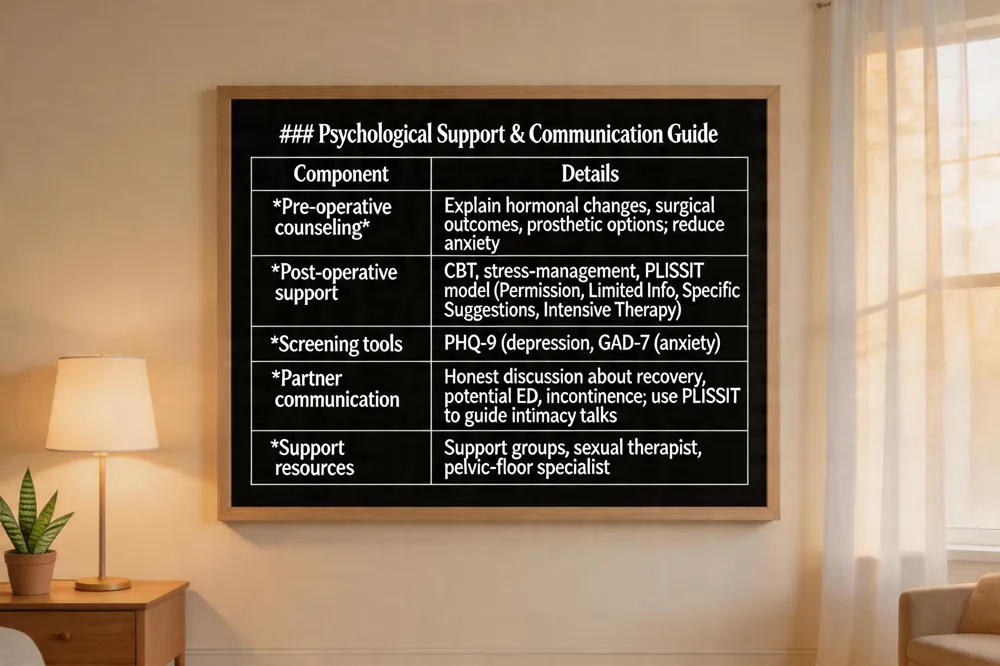 Body‑image concerns are common after orchiectomy or scrotal reduction. Pre‑operative counseling that explains hormonal changes, surgical outcomes and prosthetic options reduces anxiety and boosts confidence. Post‑operative psychological support—counseling, CBT and stress‑management—helps men cope with loss of tissue, altered appearance and mood shifts. The PLISSIT model (Permission, Limited Information, Specific Suggestions, Intensive Therapy) guides clinicians to discuss intimacy, address fears and provide tailored sexual therapy, such as pelvic‑floor exercises and PDE‑5 guidance. Mental‑health screening with PHQ‑9 and GAD‑7 detects depression or anxiety early, and support groups reduce isolation.
Answers:
- Dating after prostatectomy: Honest communication about recovery, possible erectile dysfunction, incontinence and emotional support is key.
- Psychological support after orchiectomy: Pre‑operative counseling, ongoing therapy and stress‑management lessen body‑image distress.
- Scrotal reconstruction surgery: Scrotoplasty restores shape and protection using local flaps or grafts for a natural look with minimal scarring.
- Penoscrotal webbing recovery: Wear snug support garments 2‑3 weeks, keep incisions clean and avoid vigorous activity and intercourse.
- Sleep after testicle surgery: Elevate the scrotum with a towel, wear a tight jock strap and sleep on the back for 1‑2 weeks.
- Massage after prostate surgery: Perineal or pelvic‑floor massage improves circulation and scar tissue, but only after surgeon clearance.
Resuming Intimacy: Practical Guidelines for Safe Sexual Activity
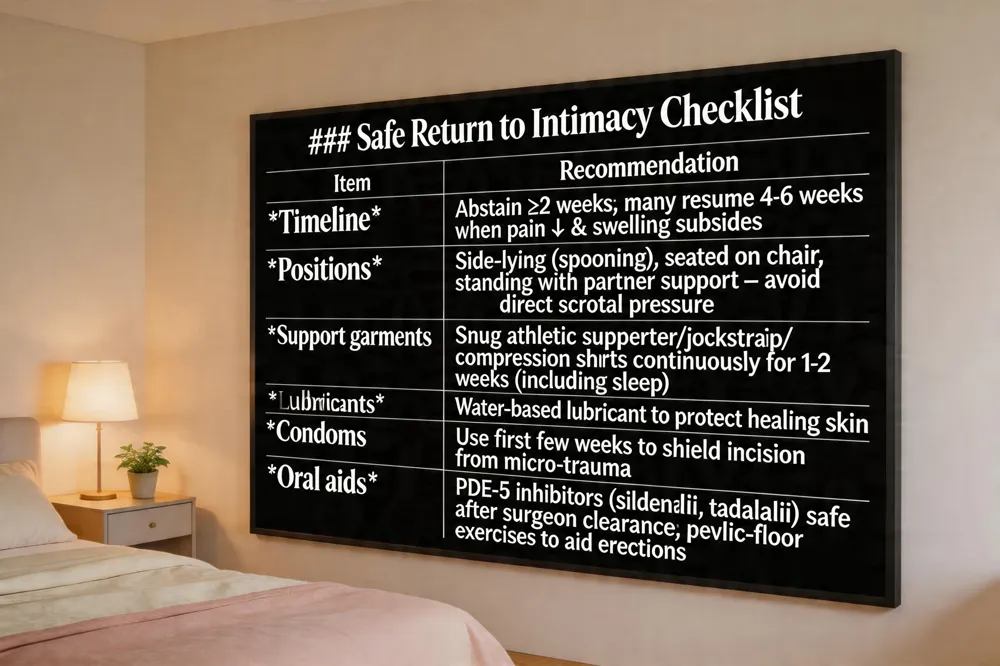 Timeline for returning to intercourse Most surgeons advise abstaining from any sexual activity for at least 2 weeks after scrotal reduction surgery, until the incisions are fully healed and cleared by the operating physician. In practice, many patients feel comfortable resuming intimacy between 4 – 6 weeks post‑op, especially when swelling has subsided and pain is minimal.
Recommended positions and protective garments During the early weeks, choose positions that keep direct pressure off the scrotum—side‑lying (spooning), seated on a chair, or standing with the partner supporting the pelvis. Wear a snug athletic supporter, jockstrap, or compression shorts continuously for the first 1‑2 weeks, even while sleeping, to keep the scrotum elevated and reduce edema.
Use of lubricants, condoms, and oral aids A water‑based lubricant minimizes friction and protects the healing skin. Condoms are advisable for the first few weeks to shield the incision from micro‑trauma. If erections are weak, oral PDE‑5 inhibitors (e.g., sildenafil, tadalafil) can be used safely after clearance, and pelvic‑floor exercises further support erectile quality.
When can you resume sexual activity after scrotal reduction surgery? Most surgeons recommend abstaining for at least 2 weeks and many patients safely resume intimacy after 4‑6 weeks.
Scrotal lift surgery cost U.S. costs range $3,000‑$10,000; most patients pay $4,500‑$7,500. Cosmetic cases are rarely covered, but medically necessary repairs may receive partial insurance reimbursement.
Scrotal lift surgery near me Search for board‑certified plastic surgeons or urologists specializing in male genital reconstruction. Dr. Victor Liu offers personalized scrotal lift procedures in the Bay Area.
Scrotal webbing surgery cost Typical fees are $2,500‑$5,000, up to $6,000 with all associated costs; financing and limited insurance options are common.
How to sleep after testicle surgery? Lie on your back with a small towel or pillow under the scrotum for elevation; wear a snug jockstrap or supportive underwear throughout the night for 1‑2 weeks.
Scrotal support after vasectomy A fitted athletic supporter, jockstrap, or specialized vasectomy recovery brief keeps the scrotum elevated, reduces swelling, and eases discomfort during the first 1‑2 weeks.
Optimizing Long‑Term Sexual Confidence
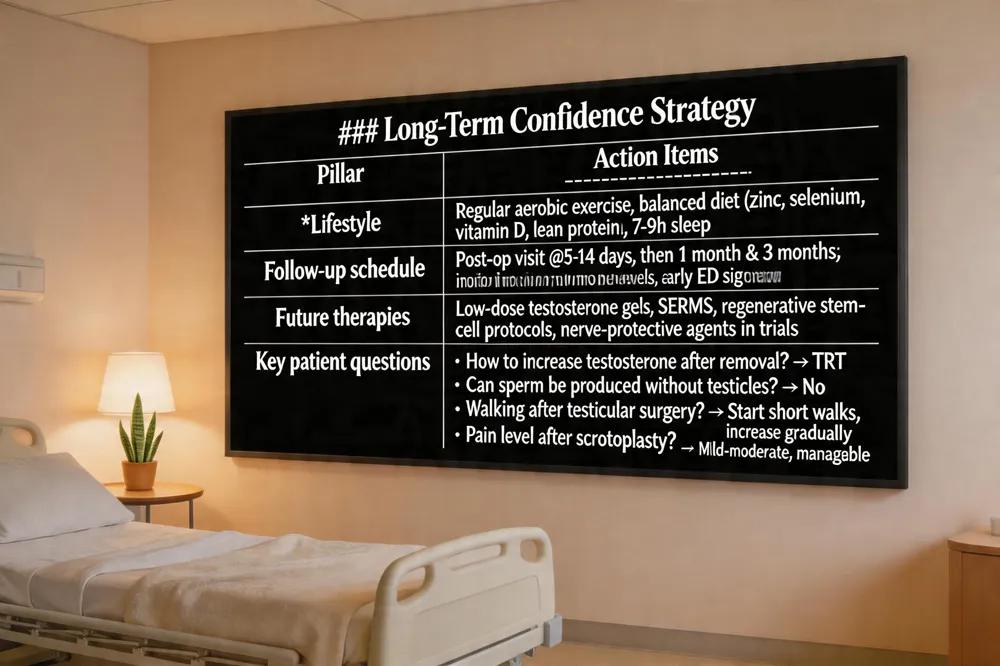 Maintaining sexual confidence after orchiectomy, scrotoplasty, or related genital surgery depends on three pillars: healthy lifestyle, vigilant follow‑up, and access to emerging therapies.
Lifestyle factors – Regular aerobic exercise (e.g., brisk walking, cycling) improves circulation, supports pelvic‑floor strength, and mitigates weight‑related scrotal sagging. A balanced diet rich in zinc, selenium, vitamin D and lean protein sustains tissue repair and testosterone‑precursor pathways; adequate sleep (7‑9 hours) regulates cortisol, which otherwise can blunt libido.
Regular follow‑up and monitoring – Schedule the first postoperative visit within 5‑14 days, then at 1 month and 3 months to assess incision healing, hormone levels, and any early signs of infection or nerve irritation. Testosterone panels guide the need for replacement therapy (TRT) when bilateral orchiectomy has occurred. Early identification of erectile dysfunction enables prompt initiation of phosphodiesterase‑5 inhibitors, vacuum devices, or pelvic‑floor rehabilitation.
Future treatments and refinements – Advances in low‑dose testosterone gels, selective estrogen‑receptor modulators, and regenerative stem‑cell protocols may further enhance libido and erectile quality. Ongoing clinical trials of nerve‑protective agents during scrotal‑reduction surgery aim to preserve sensory function and reduce postoperative dysesthesia.
Key patient questions
- How to increase testosterone after testicle removal? TRT (injections, gels, or patches) is the standard to restore normal levels.
- Can you still produce sperm with no testicle? No; sperm production stops when both testes are absent.
- Can I walk after testicular surgery? Begin with short walks, gradually increasing distance to promote circulation and prevent constipation.
- Can I poop after testicular torsion surgery? Encourage fiber‑rich foods and hydration to maintain regular bowel movements.
- How painful is scrotoplasty? The operation is painless under anesthesia; postoperative discomfort is mild‑moderate and manageable with analgesics and scrotal support.
- Scrotal webbing surgery cost Typically $2,500‑$5,000 in the U.S., up to $6,000 with all fees.
- How long does erectile dysfunction last after prostate surgery? Most men recover within the first year; nerve‑sparing techniques yield a 40‑50 % return of pre‑operative function.
Adhering to these guidelines fosters a resilient sense of sexual well‑being and long‑term confidence.
Putting It All Together: A Path to Renewed Confidence
Achieving lasting sexual satisfaction after orchiectomy or scrotoplasty requires a coordinated, multidisciplinary plan. Medically, patients should have testosterone levels checked; if low, testosterone replacement therapy (TRT) and phosphodiesterase‑5 inhibitors can restore libido and erectile quality. Physical rehabilitation includes gentle pelvic‑floor (Kegel) exercises, gradual return to aerobic activity, and the use of supportive garments or scrotal binders to protect the incision while reducing edema. Psychologically, counseling—whether cognitive‑behavioral therapy, sex‑therapy, or support‑group participation—addresses body‑image distress and performance anxiety. Partner involvement is essential: open communication, the PLISSIT model, and shared intimacy exercises foster trust and reduce self‑consciousness. Ongoing care involves regular follow‑up visits for wound assessment, hormonal monitoring, and adjustment of sexual aids. By integrating medical, physical, and emotional strategies, men can rebuild confidence, enjoy pain‑free intercourse, and sustain a satisfying sexual life long after surgery.