Why Physical Therapy Matters After Penile Surgery
After penile enlargement, grafting, or prosthesis implantation, the surgical site undergoes a cascade of tissue changes: edema, inflammation, and the inevitable formation of scar tissue that can contract and limit mobility. Early physical therapy targets these processes by promoting lymphatic drainage, maintaining microcirculation, and preventing excessive collagen deposition.
The core goals of penile rehabilitation are three‑fold: (1) preserve or restore tissue elasticity and length through gentle stretching and scar‑massage; (2) strengthen the pelvic floor (Kegel or PFMT) to improve blood flow, venous occlusion, and erectile rigidity; and (3) protect neurovascular and nerve early re‑vascularization mechanical controlled mobilization and low‑intensity shockwave therapy.
Evidence from peer‑reviewed series and systematic reviews consistently shows that structured PT shortens the time to return to normal sexual activity, reduces rates of postoperative curvature and fibrosis, and yields higher patient‑satisfaction scores. For example, supervised stretching protocols initiated 4–6 weeks post‑op have demonstrated modest gains in penile length (0.3–0.5 cm) without compromising wound integrity. When combined with adjunctive modalities such as vacuum erection devices and PDE5 inhibitors, early PT accelerates functional recovery and minimizes long‑term complications.
Foundations of Penile Rehabilitation: Edema, Scar, and Circulation
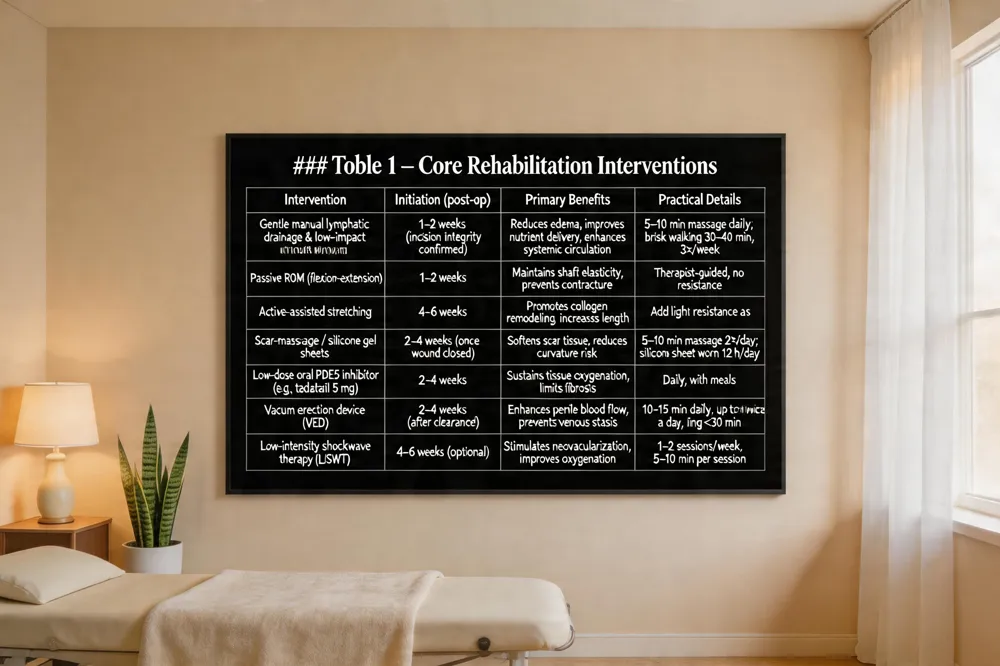 Post‑operative edema is a common response after penile enlargement or prostate‑sparing surgery. Early lymphatic drainage—gentle manual massage and low‑impact walking—helps clear excess fluid, reduces swelling, and improves nutrient delivery to healing tissues. Physical therapists typically begin these techniques within the first one to two weeks, once incision integrity is confirmed, to avoid compromising sutures.
Scar‑contracture prevention is another cornerstone of rehabilitation. Gentle manual stretching and scar‑massage protocols, often performed under professional guidance, promote collagen remodeling and maintain shaft elasticity. Silicone gel sheets or targeted myofascial release can further soften scar tissue, decreasing the risk of curvature or loss of length. A graduated program that starts with passive range‑of‑motion movements and progresses to active assisted stretching has been shown to improve patient satisfaction and functional outcomes.
Circulatory support is achieved through early mobilization and aerobic conditioning. Light cardio—brisk walking or cycling for 30‑40 minutes three times weekly enhances systemic blood flow, which directly benefits penile perfusion. Combined with low‑dose oral PDE5 inhibitors or vacuum erection devices, this approach sustains tissue oxygenation and reduces fibrosis.
Penile rehabilitation during hormone therapy – Hormone fluctuations (e.g., androgen deprivation or testosterone supplementation) can impair erectile tissue health. A personalized plan that blends low‑dose oral PDE5 inhibitors, daily vacuum‑pump sessions, and occasional intracavernosal injections preserves elasticity and oxygenation. Low‑intensity shockwave therapy may be added to boost vascular healing, all coordinated under Dr. Victor Liu’s minimally invasive protocol.
What is the best exercise for erectile dysfunction? – Targeted pelvic‑floor training, specifically Kegel (bulbocavernosus) exercises is the most effective non‑invasive intervention. Repeated 5‑10‑second holds followed by equal relaxation, performed three times daily, strengthens the muscles that regulate penile blood flow and rigidity. Variations such as rapid “flicks” and longer endurance holds further enhance control, delivering measurable improvements within weeks when combined with aerobic activity and a healthy lifestyle.
Pelvic Floor Mastery: Kegel Techniques and Their Broader Benefits
Kegel exercises for men
Kegel exercises strengthen the pelvic‑floor muscles that support the bladder, bowels, and blood flow to the penis, helping men gain better urinary control and reduce incontinence. By regularly contracting and relaxing these muscles, men can also improve erectile firmness, enhance orgasm intensity, and gain greater control over ejaculation—key factors in overall sexual performance. The routine is simple: locate the pelvic‑floor muscles by stopping the flow of urine or tightening the muscles that prevent passing gas, then squeeze for three seconds and relax for three seconds, repeating 10‑15 times per set. Aim for three sets a day, performed in different positions (lying, seated, standing) to build strength without straining the abdomen, thighs, or buttocks. Dr. Victor Liu can create a personalized, minimally invasive pelvic‑floor program that integrates Kegels with other advanced male‑enhancement treatments for safe, natural results.
Benefits of Kegel exercises for men
Kegels improve tone of the levator ani, pubococcygeus, and bulbocavernosus muscles, reducing urinary and fecal incontinence while enhancing erection rigidity and ejaculatory control. Improved pelvic‑floor tone also promotes better blood flow to the erectile tissue, alleviating prostate‑related discomfort and increasing sexual pleasure. The low‑impact nature of the exercises allows daily performance anywhere, with zero surgical risk, making them an essential component of penile rehabilitation and general male sexual health.
3 best Kegel exercises for men
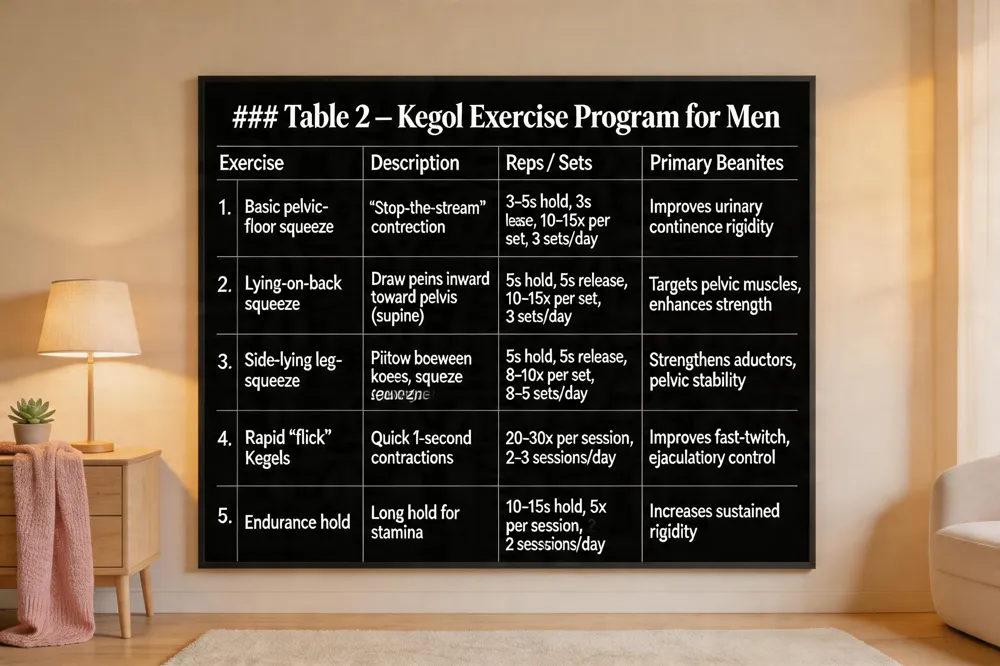
- Basic pelvic‑floor squeeze – contract the “stop‑the‑stream” muscles for 3‑5 seconds, relax same amount, repeat 10‑15 times, three sets daily.
- Lying‑on‑back squeeze – flat on back, knees bent, draw the penis inward toward the pelvis, hold five seconds, release; targets the ischiocavernosus and bulbocavernosus.
- Side‑lying leg‑squeeze – lie on side with pillow between knees, squeeze legs together for five seconds, repeat 8‑10 times, three to five sets. Consistent practice of these three variations builds pelvic‑floor strength, improves urinary continence, and enhances sexual performance.
Stretching, Scar Management, and Mobility Techniques
 Physical therapy after penile surgery is essential for preserving tissue elasticity, minimizing scar contracture, and restoring full mobility.
Gentle manual stretching and scar‑massage techniques are performed under therapist supervision to align collagen fibers and prevent excessive fibrosis. A warm‑compress before each session improves pliability, while silicone‑gel sheets or scar‑massage reduce texture and promote glide of the penile skin over underlying structures.
Progressive range‑of‑motion (ROM) protocols begin with passive flexion‑extension within 1‑2 weeks post‑op, advancing to active assisted stretching at 4‑6 weeks, and finally to active stretching with controlled resistance once wound integrity is confirmed. Gradual intensity increases protect sutures and allow safe collagen remodeling.
Adjunctive vibration and myofascial release further stimulate local circulation, break early adhesions, and accelerate healing. Low‑frequency handheld vibrators applied for 2‑3 minutes per session enhance blood flow and reduce edema, while therapist‑directed myofascial release targets dense fibrotic bands.
What exercises are good for penile rehabilitation? Pelvic‑floor strengthening (Kegels), aerobic conditioning (brisk walking, cycling), and yoga poses that increase pelvic circulation are core. Consistent practice 3‑5 times weekly supports tissue oxygenation and erectile function.
When to start penile rehabilitation after radical prostatectomy? Initiate within 2‑4 weeks post‑surgery, often with low‑dose PDE‑5 inhibitors and gentle ROM exercises, adjusting based on pain and wound healing.
Can you get hard after penile surgery? Yes; implants provide on‑demand rigidity after 4‑8 weeks of healing. Natural sensation may differ, but erections are firm and functional.
Penile implant after prostate surgery Implants are a reliable option for refractory erectile dysfunction post‑prostatectomy, offering controllable erections while preserving penile length. Dr. Victor Liu integrates personalized surgical and rehab plans for optimal outcomes.
Pelvic floor exercises following prostatectomy Begin 4‑6 weeks pre‑op or immediately post‑catheter removal with slow (5‑10 s) and fast‑twitch contractions, 3‑4 sets daily for 6‑12 months to improve continence and erectile quality.
Adjunctive Devices, Medications, and Emerging Technologies
 A modern penile‑rehabilitation program blends mechanical adjuncts, pharmacotherapy, and advanced modalities to protect tissue integrity and accelerate functional recovery.
Vacuum erection devices (VED) and low‑intensity shockwave therapy (LiSWT) – Early VED use (usually within the first few weeks after prostatectomy) promotes penile blood flow, prevents venous stasis, and limits postoperative shortening. Most clinicians prescribe a daily 10‑ to 15‑minute session, optionally repeated twice a day, with a constriction ring removed after 30 minutes. low‑intensity shockwave therapy (LiSWT) delivers focused acoustic waves that stimulate neovascularization and improve oxygenation of the corpora cavernosa, a non‑invasive adjunct shown to enhance erectile quality in post‑surgical patients.
PDE5 inhibitors, intracavernous injections, and oral agents – Daily low‑dose tadalafil (5 mg) is the preferred first‑line oral therapy for nerve‑sparing prostatectomy because it maintains continuous penile arterial inflow and supports nerve regeneration. On‑demand sildenafil or vardenafil may be added later. intracavernous alprostadil injections (twice weekly for six months) provide direct smooth‑muscle relaxation, preserving tissue health when oral agents alone are insufficient.
Biofeedback and therapeutic ultrasound – Biofeedback devices confirm correct pelvic‑floor activation during Kegel training, while low‑intensity therapeutic ultrasound reduces scar contracture and improves tissue pliability.
Key patient questions
- How often to use vacuum pump after prostate surgery? Begin after surgeon clearance, typically daily 10‑15 minutes, up to twice a day, avoiding ring wear >30 minutes. Continue 6‑12 months.
- Best pill for post‑prostatectomy ED? Daily low‑dose tadalafil (5 mg) is favored for continuous rehabilitation; on‑demand PDE5 inhibitors are alternatives.
- Speeding nerve regeneration? Combine hydration, antioxidant‑rich diet, early low‑dose PDE5 inhibitors, pelvic‑floor training, and LiSWT while avoiding smoking and excessive alcohol.
- Latest treatment for post‑prostatectomy ED? Early multimodal rehab: daily PDE5 inhibitor, scheduled intracavernous injections, VED use, and LiSWT, coordinated by a specialist such as Dr. Victor Liu.
- Can a penile pump restore function? Yes, regular VED use restores blood flow and maintains tissue elasticity, enhancing erectile outcomes when combined with other therapies.
- Time for penile nerve recovery? Initial improvements appear 3‑6 months; many men continue to recover up to 12‑24 months, with some changes persisting for two years. Early PT and metabolic health can shorten this timeline.
Putting It All Together: A Personalized Roadmap for the Bay Area Patient
 A successful rehabilitation plan begins with a thorough, individualized assessment that blends the surgeon’s operative notes with a certified male‑health physical therapist’s evaluation. The therapist tailors stretching, scar‑massage, pelvic‑floor (Kegel) protocols, and modality choices (vacuum devices, low‑intensity shockwave) to the specific surgical technique—whether lengthening, girth augmentation, or prostatectomy—while the surgeon monitors suture integrity and wound healing.
Safety requires strict adherence to pain thresholds, avoidance of excessive tension, and vigilant monitoring for infection, hematoma, or excessive edema. Progress is documented at each follow‑up, allowing intensity adjustments without compromising repairs.
Penile Rehabilitation near me – Dr. Victor Liu’s Bay Area clinic offers a comprehensive, evidence‑based program that combines minimally invasive surgery with personalized PT, VED use, and medication management. Conveniently located in the heart of the Bay Area, the practice provides seamless scheduling and multidisciplinary follow‑up.
Does penile rehabilitation work? – Structured rehab, especially when started within weeks of surgery, consistently yields higher rates of erectile recovery, reduced fibrosis, and improved penile length compared with passive healing alone. Clinical series report earlier return to sexual activity and greater patient satisfaction.
How soon can you take Viagra after prostate surgery? – Most surgeons clear PDE5‑inhibitors after catheter removal and wound closure, typically 2–4 weeks post‑op; on‑demand low‑dose trials may begin at 4–6 weeks once healing is confirmed.
What is the best exercise after prostate surgery? – Gentle daily walking coupled with supervised Kegel training offers the safest, most effective way to restore circulation, pelvic‑floor strength, and urinary continence.
How long does it take for penile nerves to recover? – Nerve recovery often begins at 3–6 months, continues through 12–24 months, and may extend to two years, depending on injury severity and adherence to rehab.
How long does turtling last after surgery? – Post‑operative fatigue varies, lasting from a few weeks to several months as the body heals.
Key Takeaways for Restoring Penile Mobility
Begin postoperative physical therapy within the first 1‑2 weeks once the surgeon clears the incision, but tailor the regimen to the specific procedure (girth augmentation, lengthening, or prosthesis placement). A balanced program blends progressive pelvic‑floor muscle training (Kegels), gentle manual stretching or scar‑massage, and low‑pressure vacuum erection devices to promote blood flow, prevent fibrosis, and maintain elasticity. Regular biofeedback or vibration adjuncts help patients apply safe force levels. Throughout rehab, maintain open dialogue with Dr. Victor Liu and his multidisciplinary team—surgeon, urologist, and certified male sexual‑health therapist—to adjust intensity, monitor for pain or infection, and ensure optimal functional and aesthetic outcomes.