Introduction to PRP and Male Genital Wellness
Platelet‑rich plasma (PRP) is an autologous blood product in which a small volume of a patient’s blood is centrifuged to concentrate platelets and their growth‑factor payload (PDGF, TGF‑β, VEGF, etc.). The concentrated plasma is then injected directly into the penile shaft, glans, or corpora cavernosa under local anesthesia, a process usually completed in less than 30 minutes. Clinicians offer PRP to men seeking improved vascular health, smoother tissue regeneration, and modest enhancement of erectile firmness, with some patients also hoping for slight girth or length gains. While the procedure is minimally invasive and generally well‑tolerated, robust evidence for permanent size increase is lacking; therefore, patients should approach PRP as a regenerative therapy aimed at tissue health rather than a guaranteed enlargement solution.
Understanding PRP and Its Biological Basis
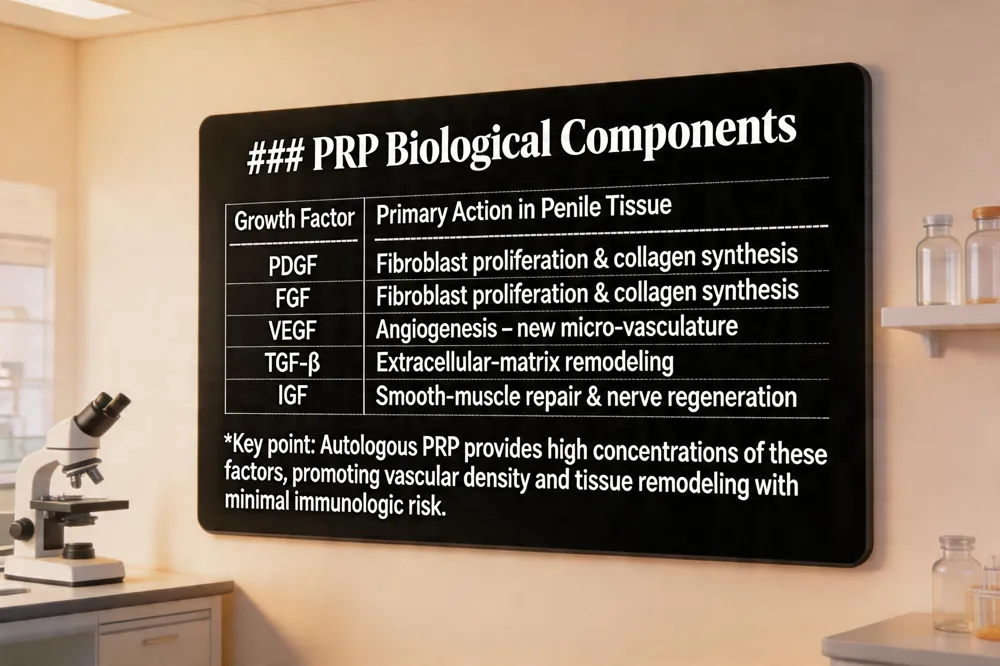 Platelet‑rich plasma (PRP) is produced by drawing a small volume of a patient’s own blood, centrifuging it, and extracting the platelet‑rich fraction. This concentrate typically contains four‑ to five‑fold higher platelet counts than baseline whole‑blood levels, delivering a potent cocktail of growth factors such as platelet‑derived growth factor (PDGF), transforming growth factor‑beta (TGF‑β), vascular endothelial growth factor (VEGF), insulin‑like growth factor (IGF), and fibroblast growth factor (FGF). These molecules act synergistically: PDGF and FGF stimulate fibroblast proliferation and collagen synthesis; VEGF drives angiogenesis, creating new micro‑vasculature; TGF‑β modulates extracellular‑matrix remodeling; and IGF supports smooth‑muscle repair and nerve regeneration. In penile tissue, this biologic activity is hypothesized to improve vascular density, enhance smooth‑muscle elasticity, and promote modest tissue remodeling. Because PRP is autologous, the risk of immunologic reaction, disease transmission, or systemic toxicity is negligible, provided strict aseptic technique is used. Minor adverse events—transient bruising, swelling, or mild discomfort—are the most common complications, while infection rates remain low when the procedure is performed by a board‑certified urologist or plastic surgeon with appropriate training.
Clinical Evidence for PRP in Erectile Dysfunction and Penile Health
Key randomized trials and systematic reviews
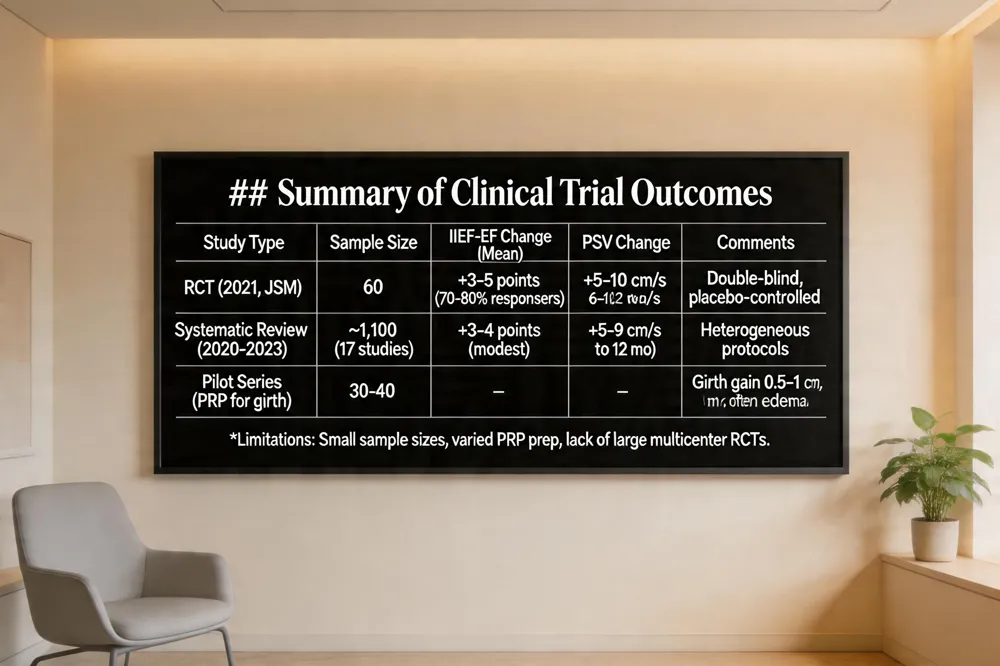
Several small‑scale, double‑blind, placebo‑controlled trials (e.g., a 60‑patient RCT published in the Journal of Sexual Medicine 2021) have shown that intracavernosal PRP injections achieve a clinically meaningful increase in International Index of Erectile Function (IIEF‑EF) scores in 70‑80 % of men versus 25‑30 % with placebo. Systematic reviews (2020‑2023) of 17 studies (≈1,100 patients) confirm modest but statistically significant IIEF improvements and gains in peak systolic velocity (PSV), while noting heterogeneity in protocols.
Observed improvements in IIEF scores and vascular parameters
Across trials, mean IIEF‑EF rises range from 3‑5 points, with corresponding PSV increases of 5‑10 cm/s, suggesting enhanced penile blood flow. Benefits typically emerge 4‑6 weeks after the final injection and may persist for 6‑12 months.
Limitations of current research and need for larger studies
Most data come from pilot series with variable PRP preparation, dosing, and follow‑up periods; no large multicenter RCTs exist. Long‑term safety and durability of size‑related outcomes remain unproven.
Does PRP actually work for men?
PRP can stimulate tissue healing and angiogenesis, offering modest functional gains for erectile dysfunction, especially when combined with lifestyle or adjunctive therapies. It is generally safe, but evidence for permanent penile enlargement is lacking; individual responses vary.
How long does PRP last for ED?
Improvement typically lasts 12‑24 months, with many clinicians recommending maintenance injections every 6‑12 months to sustain benefits.
PRP for Penile Girth and Length: What Do Studies Show?
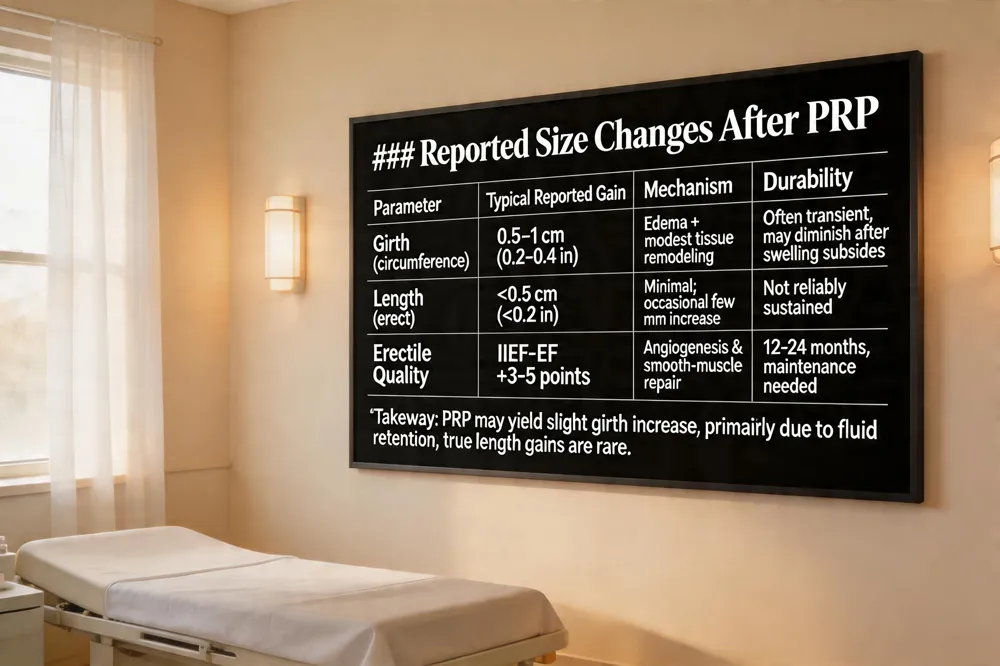 Pilot studies of platelet‑rich plasma (PRP) injections into the penile shaft have reported modest girth gains of roughly 0.5–1 cm (0.2–0.4 in) after a series of treatments, often spaced two weeks apart. These gains are inconsistent; some men experience noticeable thickening, while others observe only subtle changes. Variability appears linked to individual vascular health, the number of sessions, and whether PRP is combined with adjunctive modalities such as vacuum erection devices or penile traction therapy. In many cases the early increase in girth is largely due to transient edema and fluid accumulation rather than true tissue remodeling; true growth, if it occurs, tends to be modest and may diminish once swelling subsides.
Does PRP add girth? Yes, PRP can produce a slight increase in girth for many men by promoting angiogenesis and tissue repair, especially when paired with enhanced blood flow from adjunctive therapies. Results are variable and depend on anatomy, treatment frequency, and protocol.
How many inches does the P‑Shot add? Length gains are uncommon; most men see little or no change. When an increase does occur, it is usually less than an inch, often only a few millimeters, and is not guaranteed. The primary benefit are improved erectile quality and sensation, not dramatic size augmentation.
Cost and Practical Considerations of the P‑Shot
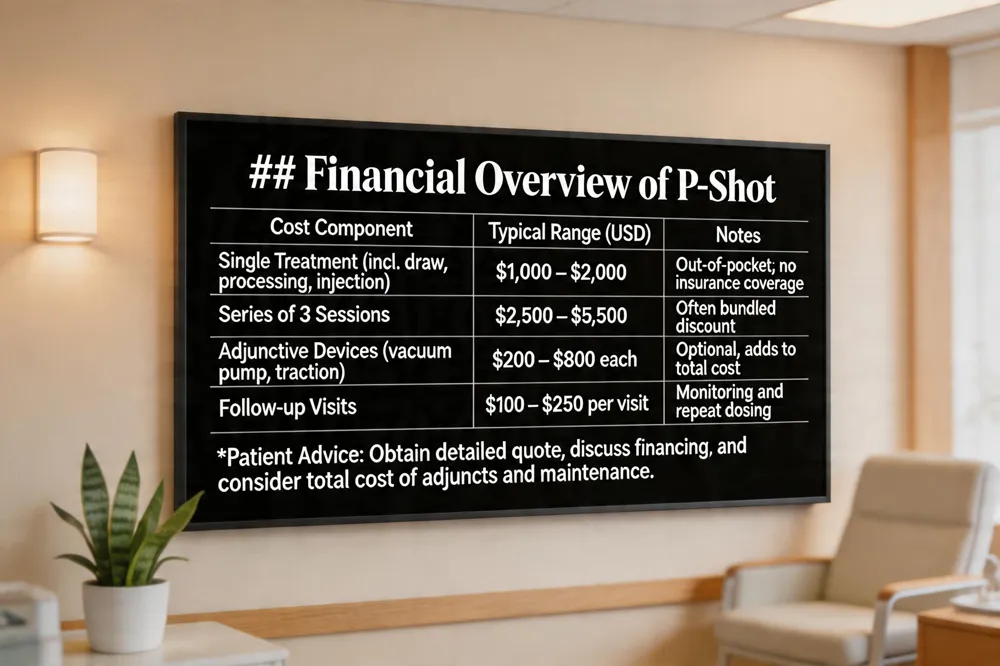 The Priapus Shot (P‑Shot) is an out‑of‑pocket procedure that typically costs $1,000 – $2,000 per treatment. This fee usually covers the venous blood draw, centrifugation, processing of platelet‑rich plasma, local anesthesia, and the injection itself. Health‑insurance plans do not cover the P‑Shot, as it is classified as an experimental, off‑label use of autologous PRP. Total cost can rise when clinics add adjunctive devices (e.g., daily vacuum pumps or penile traction therapy), request multiple injection sessions, or schedule follow‑up visits for monitoring and repeat treatments. The volume of PRP prepared, the number of injection sites, and any bundled packages (e.g., a series of three sessions) also influence the final price. Patients should obtain a detailed quote and discuss financing options before proceeding.
Comparing Surgical and Non‑Surgical Options: Penuma Implant vs PRP
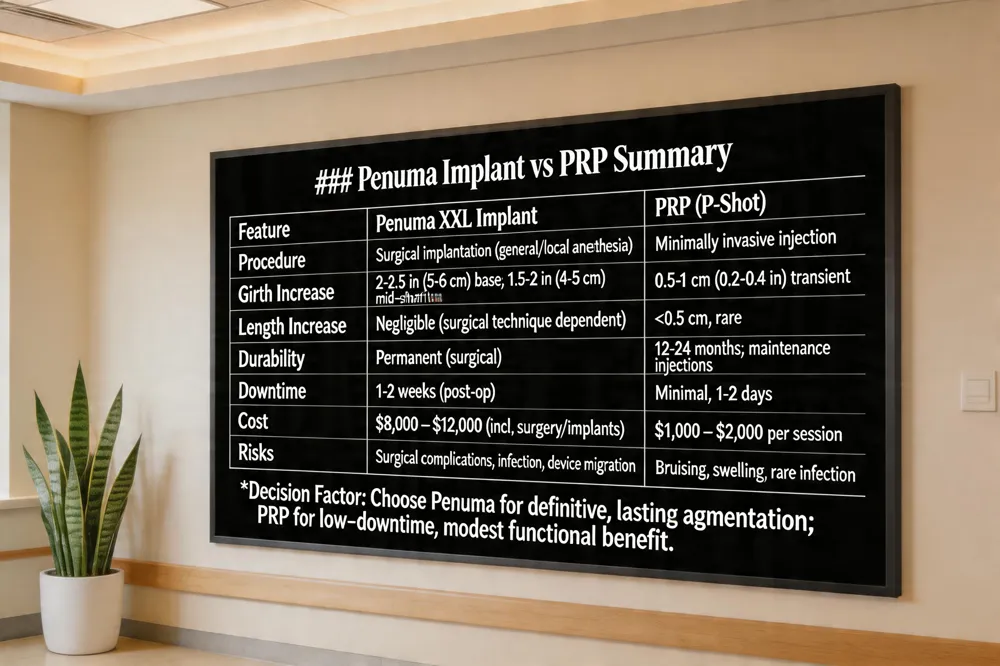 The Penuma XXL implant is the largest device in the Penuma line and typically adds 2 to 2.5 inches (5 – 6 cm) of girth at the penile base, with a slightly smaller increase of 1.5 to 2 inches (4 – 5 cm) at the mid‑shaft. This gain is measured as an increase in circumference, not diameter, and varies with individual anatomy and surgical technique.
Surgical placement offers a permanent, predictable augmentation that can be precisely sized to the patient’s goals, providing a stable, natural‑feeling result that does not require repeated sessions. In contrast, injectable PRP (the P‑Shot) is a minimally invasive, off‑label therapy that relies on autologous growth factors to promote tissue health. While PRP may modestly improve erectile function and, in some small pilot studies, yield transient girth gains of 0.5–1 cm, the evidence for lasting size enhancement is weak and outcomes are highly variable.
Patient selection is critical: men seeking a definitive, long‑term increase in girth and who are good surgical candidates are ideal for Penuma, whereas those preferring a non‑surgical, low‑downtime option with modest, experimental benefits may consider PRP after thorough counseling on realistic expectations.
Normal Penis Size: Setting Realistic Expectations
 Meta‑analysis averages for flaccid and erect lengths and circumferences show that the typical male penis falls within a relatively tight range. A large pooled analysis of 15,521 men found a mean flaccid length of 9.2 cm (3.6 in) and a mean erect length of 13.1 cm (5.2 in). Corresponding circumferences average 9.3 cm (3.7 in) flaccid and 11.7 cm (4.6 in) erect. Percentile distribution places a 10 cm (4‑in) erect penis at the 5th percentile and a 16 cm (6.3‑in) erect penis at the 95th percentile, indicating that the majority of men lie between these limits. Concerns about size can erode sexual confidence, yet size alone does not predict performance or satisfaction. When anxiety arises, clinicians should offer evidence‑based counseling and, if appropriate, safe, personalized treatment options that address functional goals rather than unrealistic expectations of dramatic growth.
Choosing a Qualified Provider and Personalized Treatment Planning
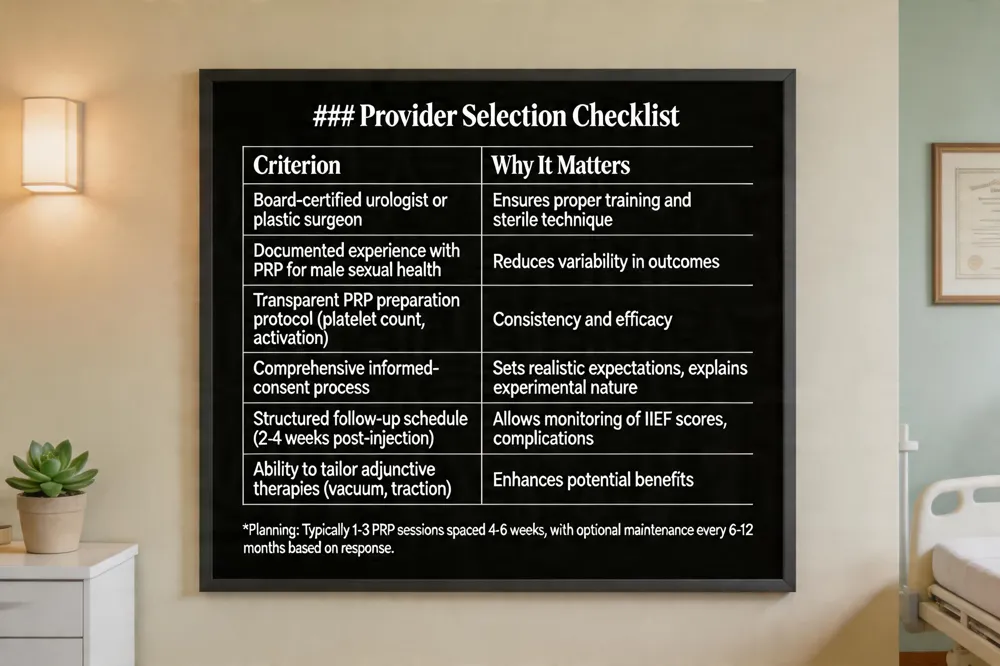 When considering platelet‑rich plasma (PRP) injections for penile health, the most critical decision is selecting a board‑certified urologist or plastic surgeon with documented expertise in male sexual‑medicine. Certified such as Board.cert Liuurologist Liu ( board are a physiciansocaly can surgeons have‑‑ experience** performed and series and In and ascar the Hands assessment‑ P‑Shot. Their training ensures adherence to sterile technique, proper PRP preparation (including platelet concentration and activation), and accurate injection of the base, shaft, or glans.
Informed consent and pre‑procedure evaluation are essential. A qualified provider will review the patient’s medical history, rule out contraindications (e.g., uncontrolled diabetes, active infection, coagulopathy), and discuss realistic expectations—current evidence shows only modest, short‑term improvements in erectile function and no reliable data for permanent length or girth gain. The consent form should outline the experimental nature of the procedure, off‑label status, potential minor adverse events (bruising, swelling, infection), and the out‑of‑pocket cost, which typically exceeds $1,000 per session.
Personalized treatment planning includes determining the number of PRP injections (often 1–3 sessions spaced 4–6 weeks apart), optional adjuncts such as vacuum devices, and a structured follow‑up schedule. Follow‑up visits, typically 2–4 weeks after each injection, allow the clinician to assess erectile function scores (e.g., IIEF), monitor for complications, and decide whether maintenance injections are warranted. By choosing an experienced, board‑certified specialist and engaging in a thorough, evidence‑based counseling process, men can pursue PRP therapy with confidence in safety and appropriate clinical oversight.
Conclusion: Informed Decisions for Natural Penile Enhancement
Current data show that platelet‑rich plasma (PRP) injections are safe when performed under sterile conditions, with only mild bruising, swelling or transient discomfort reported. However, robust randomized trials demonstrating reliable improvements in erectile function, penile length or girth are lacking; most studies are small, uncontrolled and produce modest, short‑term changes that may reflect tissue edema rather than true growth. For men seeking more pronounced girth augmentation, surgical options such as the Penuma subcutaneous implant provide documented increases of 4–8 cm in circumference, but they carry higher rates of infection, scarring and require anesthesia. Regardless of the chosen modality, patients should maintain realistic expectations, understand that results can vary, and commit to regular follow‑up with a board‑certified urologist or plastic surgeon experienced in male sexual health to monitor outcomes and address any complications promptly effectively.